|
Sarafem
By S. Jensgar. Baldwin-Wallace College.
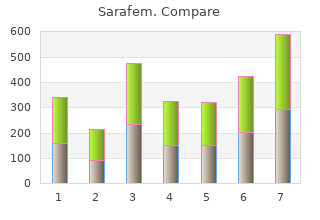
This served merely as a proof of concept at this stage best sarafem 10 mg pregnancy, and more extensive or proprietary toxicity predictors could readily extend or replace this component order sarafem 10 mg free shipping womens health professionals. For energy 179 Chapter 6 calculation, the minimized energy of a single 3D conformer was used (note that until this point, only the topology (‘graphs’) of the molecules was considered). Occurrence of high-energy structures, which were weeded from the total compound library, is a consequence of the random modification of the molecular graph, which may result in less feasible molecules. Flow chart of the evolutionary optimization loop (see Experimental for detailed explanation). After the initial generation and filtering phase, the ‘fittest’ molecules were selected to serve as parents for the subsequent generation. We 180 Multi-Objective Evolutionary Ligand Design chose to replicate this pharmacophore model because it proved successful for the design of novel ligand chemistry with sufficient specificity. Visual representation of the pharmacophore model used to search for 13 A1 ligands, based on a previously reported pharmacophore. The aromatic core is represented by three spheres F5, F7, and F9, and three spheres that indicate the direction of the normal of the aromatic feature, F6, F8, and F10. At least one of the aromatic features with normal projection should be occupied by a corresponding aromatic feature in the molecule. A hydrogen bond acceptor and donor region are represented by F1 and F3, respectively. The grey dots indicate the inclusion volume, the volume into which the molecules generated need to fit for not being subject to a fit penalty. The reason for this is that for the adenosine A1 receptor the binding features needed to be defined as specific as possible, while for the other three subtypes (selectivity score) a broad range of possible ligand features had to be detected to ensure selectivity. Property ranges were defined, outside of which molecules were rejected using filters. For this, each property was converted using a desirability function to a value between zero and one, where zero (0) indicates undesirable property values and one (1) that property values are excellent. The use of desirability 15 functions/indices originates from areas such as quality control. This was performed with Pareto selection, which is a method to select the best candidates 16 when considering multiple objectives. In contrast to a simple combination of scores into a single score, Pareto selection considers all three scores simultaneously to select the best candidates. Since evolutionary algorithms have a tendency to focus towards 17 small regions of the chemical search space, diversity of the parent molecules was 18 also taken into account using niching. Niching enforces diversity within populations of candidate solutions by maintaining separated groups, requiring a minimum distance between those groups and a maximum distance between the group members. For each new generation, the number of known structures, the number of structures with known adenosine ligand scaffolds, and the number of structures with high 182 Multi-Objective Evolutionary Ligand Design pharmacophore score were calculated. Chart 1 shows the percentage of compounds that contain known adenosine scaffolds as well as those having a high pharmacophore score. The occurrence of scaffolds also found in adenosine ligands (which were removed) gave us some upfront confidence that the generated structures might indeed be potential adenosine receptor ligands. In general, the number of compounds with a high pharmacophore score is expected to improve over the generations while the number of unknown compounds will increase as well. Although generation of novel compounds is preferred from a medicinal chemistry point of view, a high number of unknown compounds also signals for potential difficulties with synthesis planning or acquisition of starting materials. As visualized by the ‘Scaffolds’ bars in Chart 1, the percentage of scaffolds also found in common adenosine receptor ligands decreases with each generation. The data presented in Chart 1 also suggests that the pharmacophore fit improves with each subsequent generation; the first generated compounds with at least 13 pharmacophore matches first appear in the fifth generation. Percentage of compounds that contain known adenosine ligand scaffolds (“Scaffolds”), and the percentage of compounds with at least 11, 12, or 13 pharmacophore feature hits (“Hits11”/”Hits12”/”Hits13”) per generation (number of generations on X-axis). The generated molecules from all generations were collected and merged into one set (discarding duplicates), resulting in a set of 3.
Which rationale best justifies administering different antitu- bercular drugs concurrently in treating active tuberculosis? Combination therapy can prevent or delay bacterial resistance to antitubercular drugs cheap 10 mg sarafem with amex women's health center unm. Today’s lesson includes information Immune and inflammatory responses protect the body from invad- about drug classes ing foreign substances buy 10 mg sarafem otc womens health zinc. These responses can be modified by cer- that can modify tain classes of drugs: responses. Histamine-1 receptor antagonists The term antihistamine refers to drugs that act as histamine-1 (H1) receptor antagonists; that is, they compete with histamine for binding to H1-receptor sites throughout the body. It’s all about chemistry Based on chemical structure, antihistamines are categorized into five major classes: • Ethanolamines include clemastine fumarate, dimenhydrinate, and diphenhydramine hydrochloride. Pharmacokinetics (how drugs circulate) H1-receptor antagonists are well absorbed after oral or parenteral administration. Pharmacodynamics (how drugs act) H1-receptor antagonists compete with histamine for H1 receptors on effector cells (the cells that cause allergic symptoms), blocking histamine from producing its effects. These drugs include diphenhydramine, dimenhydrinate, promethazine, and various piperidine derivatives. No stomach for this H1-receptor antagonists don’t affect parietal cell secretion in the stomach because their receptors are H2 receptors, not H1. The first one there wins Release the mediators Chlorpheniramine competes with histamine for H1-receptor When sensitized to an antigen, a mast cell reacts to repeated sites on the effector cells. By attaching to these sites first, the antigen exposure by releasing chemical mediators. Not just for allergies Antihistamines can have other therapeutic uses: Adverse • Many are used primarily as antiemetics (to control nausea and vomiting). The most common ad- • Diphenhydramine can help treat Parkinson’s disease and drug- verse reaction to anti- induced extrapyramidal reactions (abnormal involuntary move- ments). They can get the heart racing Corticosteroids Cardiovascular reac- tions may include: Corticosteroids suppress immune responses and reduce inflam- • hypotension mation. Natural and synthetic corticosteroids are classified ac- Sensitivity reactions can cording to their biological activities: also occur. Glucocorticoids Most glucocorticoids are synthetic analogues of hormones secret- ed by the adrenal cortex. Drugs in this class include: • beclomethasone • betamethasone • cortisone • dexamethasone • hydrocortisone • methylprednisolone • prednisolone • prednisone • triamcinolone. Distribution Glucocorticoids are bound to plasma proteins and distributed through the blood. Unfortunately, Metabolism and excretion when glucocorticoids inhibit the immune Glucocorticoids are metabolized in the liver and excreted by the response they may kidneys. Glucocorticoids suppress hypersensitivity and immune responses through a process that isn’t entirely understood. Researchers be- lieve that glucocorticoids inhibit immune responses by: • suppressing or preventing cell-mediated immune reactions • reducing levels of leukocytes, monocytes, and eosinophils • decreasing the binding of immunoglobulins to cell surface re- ceptors • inhibiting interleukin synthesis. Taking the red (and more) out Glucocorticoids suppress the redness, edema, heat, and tender- ness associated with the inflammatory response. How methylprednisolone works Tissue trauma normally leads to tissue irritation, edema, inflammation, and production of scar tissue. Methylprednisolone counter- acts the initial effects of tissue trauma, promoting healing. No leaks, no drips As corticosteroids, glucocorticoids prevent the leakage of plasma from capillaries, suppress the migration of polymorphonuclear leukocytes (cells that kill and digest microorganisms), and inhibit phagocytosis (ingestion and destruction). To ensure a job well done, glucocorticoids decrease antibody formation in injured or infected tissues and disrupt histamine syn- thesis, fibroblast development, collagen deposition, capillary dila- tion, and capillary permeability. Adverse reactions to corticosteroids Corticosteroids affect almost • suppressed immune and in- • diabetes mellitus all body systems. Their wide- flammatory responses • hyperlipidemia spread adverse effects in- • osteoporosis • adrenal atrophy clude: • intestinal perforation • hypothalamic-pituitary axis • insomnia • peptic ulcers suppression • increased sodium and wa- • impaired wound healing. Drug interactions Many drugs interact with corticosteroids: • Aminoglutethimide, barbiturates, phenytoin, and rifampin may reduce the effects of corticosteroids.
In addition to more traditional categories of knowledge order sarafem 10 mg online menstrual questionnaire, such as knowledge on procedures and processes order sarafem 20 mg mastercard breast cancer 5k harrisonburg va, and basic and clinical knowledge, we fnd two less traditional and contrary categories, the living and the inert. The differential principles of action may also explain the absence of any hierarchization of knowledge; procedural and process 303 Catherine Garnier knowledge is as important as the very specialized knowledge regarding the ultimate purpose of the research. The chronologies The event chronologies were analyzed on the basis of two different sources, the scientifc publications and a press review. In terms of their effect on cancer, the substances are found to be effective, and in terms of sources of information, the majority comes from university research centres. It should, however, be noted that, for Vioxx, the frst published data come mainly from Merck, the company that produced the drug. In the light of these observations and the crisis related the withdrawal of Vioxx from the market, certain questions arise. To what extent does the research carried out before a drug is approved address all the risks suffciently? To what degree does it do so, given that the frst part of the chronology provides little information on the harmful or side effects of the medications? In any event, there are limits to the diversity of the populations involved in clinical trials and to the duration of such trials, so these two dimensions necessarily give rise to some uncertainty. The Vioxx chronology, derived from the abstracts of scientifc studies, does not really allow us, at this stage, to predict crises like those sparked by the withdrawal of the drug. Still, the difference between the chronologies of these substances brings out the fact that plant- and animal-derived extracts are not on the same level as prescription medications. In the case of the plant and animal extracts, almost all that has to be shown is that they are effective in a particular area. In the case of prescription drugs, it is also essential to demonstrate that they are not harmful or, at least, that the contributions they are likely to make outweigh any of their toxic aspects. Information from the abstracts is indicated in the fgure in accordance with its importance in the chronology of the medication: events of moderate importance are shown at a medium distance from the timeline, and events of major importance (withdrawal or approval of the drug, lawsuit or important discovery, etc. Each circle of the fgure thus represents an event referring to a scientifc abstract or a news item. It should be noted that, as far as news items from dailies are concerned, redundant references to the same event were not considered. Furthermore, events were positioned according to their valence: that is their positive (above the timeline) or negative (below the timeline) impact on the future of the drug. Lastly, for the fgure involving news from the dailies, coloured lines were added to the timeline to indicate critical incidents; that is events marking the pathway of the medication (for instance, approval, withdrawal, lawsuits, discovery of major side effects, etc. In the case of information drawn from Medline, the coloured lines represent the dimensions under study (pharmacological properties, particular indication, etc. This distinction probably stems from the fact that, in contrast to the other three substances, Vioxx is the only one to have been marketed. This observation must however be qualifed by stating that, for the most part, negative incidents emerge only after a medication is approved. The fact that negative information is generally produced by university research centres and regulatory agencies gives rise to two concerns. First, once a medication is marketed, it seems to be up to institutions with no economic interest in the drug to reveal any risks taking it may entail. Second, there are questions about the evaluation methods, at least with regard to the duration of clinical trials in relation to the types of populations involved in them. Instead of issuing a full approval, there would be progressive measures, adjusted on the basis of specifc studies by researchers related to the time and population factors. Conclusion All our analyses tend to point up the diversity of types of knowledge that are actualized in the laboratory, even though the refocusing on the object of research is a permanent fact of life and is largely supported by the social conditions of the production of knowledge. There also emerges from the analysis a concern for crosspollination that is refected in the importation of resources from other felds – a process particularly well illustrated by the reconstruction of the networks of actors – so that the production of knowledge does not dry up as a result of the contraction of the object of specialization. One cannot help thinking of the metaphor that arose frequently in the discourse of the researchers during interviews in these laboratories regarding the drying up of the tumour, starving it by sabotaging the development of the blood vessels that proliferate to feed it.
Stigma can also attract troubled young people; which probably explains why many drug prevention programmes paradoxically lead to more discount sarafem 20 mg free shipping breast cancer ribbon clipart, rather than less cheap 10 mg sarafem free shipping women's health clinic umich, drug use. This can progress to increasing isolation, disrupted relationships with family, and loss of social supports. All these factors contribute to the development of the ‘addict identity’ – someone who has become conditioned to see himself existing outside of normal society, isolated and defiant. Once in treatment, and able to stop compulsive drug use, it is not rare for the patient to sabotage his own treatment, for example by dropping out, or missing scheduled appointments, taking refuge in the familiar experience of failure, disapproval and conflict. There is a major element of behavioural treatment in how doctors, nurses and pharmacists respond to the challenge of disaffected, impulsive behaviour. Clinics delivering the same ‘treatment’ often achieve dramatically different outcomes, and the quality of the therapeutic relationship is one factor contributing to the greater effectiveness observed in some settings. Managing addiction involves long-term support, educating patients about their condition, promoting engagement in and compliance with treatment, monitoring symptoms and dealing with complications. Practitioners treating drug-dependent patients require not just skills and knowledge, but also a positive attitude towards treatment and recovery. Negative attitudes on the part of drug-dependent patients may sabotage treatment, but so too can negative attitudes on the part of practitioners. Their theme was that, freed from the cycle of addiction and treated with respect and dignity, heroin users can develop a different image of themselves, and behave with self-respect and dignity. They emphasised that negative assumptions about drug users need to be balanced by a belief in their capacity to change, and a sense of the practitioner’s role in fostering that change. From the mid 1990s, neuroscience research has been promoted as showing that addiction is a ‘chronic relapsing brain disease’ (see Section 1. The secondary school he attended recognised that he had learning difficulties and he was sent to a boarding school for children with special needs. Within two years he was addicted to heroin, spending £150 to £200 daily on the drug, gaining the money by begging, thieving and raiding phone boxes and parking meters. He acquired an extensive criminal history, including five periods of imprisonment. In 2007, again homeless, he was picked up by another community drug project and placed in a hostel. Here, diamorphine (pharmaceutical heroin) is prescribed for patients not responding to oral methadone. Administration of diamorphine is all supervised by trained staff, and the service users attend twice daily and engage in frequent reviews and keyworking (see Glossary) sessions. For the first several months he remained chaotic and disorganised, often missing doses and continuing to use street drugs. In August 2011, although continuing to smoke crack about twice per month, he had ceased illicit heroin use, and his personal hygiene, mood and outlook had improved dramatically. He acquired a publicly funded flat, and began occupational therapy sessions to improve his literacy. His primary reaction is surprise that he has made such a vast improvement in his life. Criminal sanctions were no deterrent to his drug-using career, and he did not respond to methadone. At present, his downward spiral has been interrupted and reversed by diamorphine treatment. The continuing challenge is to build a sustainable recovery, based on self-care in stable housing and gaining employment. That would provide a basis for progressively reducing his frequency of injecting, and eventually returning to oral medication. Prescribing diamorphine for heroin addicts is a poorly understood, often controversial, modality of treatment. This case history is presented to illustrate some of the reasons why prescribing diamorphine can have advantages over other treatment approaches. Opioid substitution therapy is the prescribing and administration of a pharmaceutical opioid as a ‘substitute’ for illicit opioids, to patients who have become dependent. Clear rules and expectations of behaviour, enforced consistently, offer a new (and sometimes challenging) experience for previously asocial or antisocial individuals.
Despite three decades of intensive research on liposomes as drug delivery sys- tems best sarafem 20 mg breast cancer treatments, the number of systems that have undergone clinical trials and then reached the market has been quite modest buy generic sarafem 20 mg on-line menstruation on full moon. Furthermore, the scientific community has been skeptical that such goals could be achieved, because huge investments of funds and promising research studies have frequently ended in disappointing results or have been slow to yield successfully marketed therapeutic dosage forms based on lipid nanotechnology. Thus, the focus of the research activity has shifted to nanopartic- ulate drug delivery systems, as there are still significant unmet medical needs in target diseases such as cancer, autoimmune disorders, macular degeneration, and Alzheimer’s disease. Most of the active ingredients used to treat these severe dis- eases can be administered only through the systemic route. Indeed, both molecular complexity associated with drugs and inaccessibility of most pharmacological tar- gets are the major constraints and the main reasons behind the renewed curiosity and expanding research on nanodelivery systems, which can carry drugs directly to their site of action. Ongoing efforts are being made to develop polymeric nanocarri- ers capable of delivering active molecules specifically to the intended target organ. This approach involves modifying the pharmacokinetic profile of various therapeu- tic classes of drugs through their incorporation into nanodelivery systems. These site-specific delivery systems allow an effective drug concentration to be maintained for a longer interval in the target tissue and result in decreased adverse effects asso- ciated with lower plasma concentrations in the peripheral blood. Thus, drug tar- geting has evolved as the most desirable but elusive goal in the science of drug nanodelivery. Increased knowledge on the cellular internalization mech- anisms of the nanocarriers is crucial for improving their efficacy, site-specific deliv- ery, and intracellular targeting. Optimal pharmacological responses require both spatial placement of the drug molecules and temporal control at the site of action. Many hurdles still need to be overcome through intensive efforts and concentrated interdisciplinary scientific collaborations to reach the desired goals. However, in recent years, efforts have started to yield results with the approval by health author- ities of nanoparticles containing paclitaxel (Abraxane r ) for improved cancer ther- apy, which has rapidly become a commercial success. A large number of clinical trials are currently underway and are again raising the hopes and interest in drug nanodelivery systems. There are various techniques to prepare drug-loaded nanoparticles, the selection of which depends on the physicochemical properties of the bioactive molecule and the polymer. The nanoparticulate drug delivery field is complex and requires con- siderable interdisciplinary knowledge. Yashwant Pathak co-edited their first book in a series on nanoparticulate drug delivery systems, which was pub- lished by Informa Healthcare in 2007. The book covered recent trends and emerging technologies in the field and was very well received by the scientific community. Thassu are covering various aspects of the field with a focus on formulations and characterization—two crucial but poorly understood issues in this technology. Chapters 1 to 11 cover various for- mulation aspects of nanoparticulate drug delivery systems. They embrace delivery of small molecules, macromolecules like therapeutic proteins, applications in gene therapy, and drug delivery systems for cancer, diabetes treatment, dermal appli- cations, and many more. Chapters 12 to 15 cover the in vitro and in vivo evalua- tion as well as characterizations of the nanoparticulate drug delivery systems. The remaining chapters describe various analytical techniques used for the character- ization of nanomaterials with special reference to nanomedicines. Thus, a better understanding of physicochem- ical and physiological obstacles that a drug needs to overcome should provide the pharmaceutical scientist with information and tools needed to develop successful designs for drug targeting delivery systems. The book is therefore a timely publica- tion that provides an opportunity for scientists to learn about the complex develop- ment issues of nanoparticulate drug delivery systems. The book clearly and comprehensively presents recent advances and knowledge related to formulation and characterization of nanoparticulate drug delivery sys- tems and is an excellent reference for researchers in the field of nanomedicine. Deepak Thassu are to be complimented for both their judicial choice of topics in nanodelivery systems and their characterization techniques as well as for their selection of such respected and expert contribu- tors from the field. Pathak and Thassu through their book will contribute to Foreword xi advancements in designing and successfully developing new generations of nan- odelivery systems. Simon Benita The Institute of Drug Research School of Pharmacy The Hebrew University of Jerusalem Jerusalem, Israel Preface Modern nanotechnology is an emerging and dynamic field. It appears that Mother Nature was the first scientist offering nanoscale materials abundantly and they were used by the human beings from time immemo- rial. Several ancient practices have been developing nanoparticles through the tra- ditional processes but these were not identified as nanosystems or nanoparticles.
In mice cheap sarafem 10mg without prescription womens health clinic las vegas, the pharmacokinetics of teniposide differs from that of etoposide cheap sarafem 20 mg with visa menstruation history, a closely related drug, with lower clearance, a larger volume of distribution and a longer terminal elimination half-time. The accumulation of teniposide in leukaemic cells in vitro was some 15 times higher than that of etoposide applied at the same concentration. The major dose-limiting toxic effect of teniposide in clinical trials is myelo- suppression, manifest mainly as leukopenia. Less severe effects, including nausea and vomiting, diarrhoea and alopecia, are common; less common effects include transient increases in liver enzyme activity, hypertension and hypersensitivity reactions. Embryo- toxicity and teratogenicity, especially in the heart and central nervous system, have been observed in mice. Teniposide is orders of magnitude more toxic in mammalian than in microbial cells and is mutagenic in mammalian cells. There is inadequate evidence in experimental animals for the carcinogenicity of teniposide. In reaching this conclusion, the Working Group noted that teniposide causes distinctive cytogenetic lesions in leukaemic cells that can be readily distinguished from those induced by alkylating agents. The short latency of these leukaemias contrasts with that of leukaemia induced by alkylating agents. High-performance liquid chromatography is the most useful analytical tool for analysing mitoxantrone and its metabolites in biological matrices. Ion-pair chromato- graphy and radioimmunoassay have also been used (Beijnen et al. This product is aromatized with chloranil as the oxidant, and it is converted into mito- xantrone hydrochloride by treatment with hydrogen chloride in ethanol (Beijnen et al. Mitoxantrone, a dihydroxyanthracenedione derivative, was the most active of a series of compounds synthesized (Zee-Cheng & Cheng, 1978; Dunn & Goa, 1996). It was found to have anti-tumour activity in advanced breast cancer (often in patients in whom other treatments have failed), non-Hodgkin lymphoma and certain leukaemias. It is still most commonly used in these tumours, typically in combination with other cytotoxic drugs, and has also been used in the treatment of other cancers such as ovarian, prostate and lung cancer (Faulds et al. The typical dose is the equivalent of 12–14 mg/m2 mitoxantrone once every three weeks in patients with lymphomas and tumours of solid tissues, and 12 mg/m2 per day for five days in patients with leukaemia. When mitoxantrone is used in combination with other cytotoxic drugs, these doses are often lower (Dunn & Goa, 1996; Royal Pharmaceutical Society of Great Britain, 1999). In recent years, mitoxantrone has been used to a limited extent in the treatment of multiple sclerosis, typically at doses lower than those used in malignant disease and on a monthly schedule (Gonsettte, 1996; Millefiorini et al. Studies of Cancer in Humans The Working Group considered only studies in which mitoxantrone was given to patients who did not receive treatments with alkylating agents, with the exception of low doses of cyclophosphamide. A woman, 51 years old, with a primary breast tumour had received a combination of mitoxantrone, vincristine, 5-fluorouracil, cyclophosphamide and radiotherapy (chest and axillary); she developed acute promyelocytic leukaemia nine months later. The first case was that of a woman (aged 56 years) who received eight cycles of mitoxantrone (7 mg/m2), metho- trexate and mitomycin, local radiotherapy to the breast and axilla and tamoxifen. The second patient (aged 39 years) was also treated with eight cycles of mitoxantrone (7 mg/m2), methotrexate and mitomycin and in addition received radiotherapy to the breast. They had previously received radical mastectomy and either cyclophosphamide, metho- trexate and 5-fluorouracil or radiotherapy or both. Treatment with methotrexate, mito- xantrone and mitomycin was followed by tamoxifen, medroxyprogesterone acetate or medroxyprogesterone acetate and radiation therapy. Acute myeloid leukaemia (one case of acute monoblastic leukaemia, one of acute promyelocytic leukaemia and one of acute undifferentiated leukaemia) occurred 12–30 months after the start of treatment with the mitoxantrone-containing regimen. The patient had been treated with high doses of corticosteroids during exacerbation of the multiple sclerosis. Five years before the diagnosis of acute promyelocytic leukaemia, the patient had received an intravenous dose of mitoxantrone (10 mg/m2) once a month for five months (total dose, 87. The patient was reported to have no history of exposure to known leukaemogenic risk factors or a personal or family history of malignancy. Partridge and Lowdell (1999) reported the development of myelodysplastic syndrome in a 62-year-old woman treated for advanced breast cancer with five courses of mitoxantrone (7 mg/m2), methotrexate and mitomycin. In addition, she had received radiotherapy to the breast and axilla and tamoxifen. The planned doses for the intravenous regimen that included mitomycin (n = 30) were: mitoxantrone, 8 mg/m2 every three weeks (total dose, 64 mg); mito- mycin, 8 mg/m2 every six weeks (total dose, 32 mg) and methothrexate, 30 mg/m2 every three weeks (total dose, 240 mg). The planned doses for the intravenous regimen that did not include mitomycin (n = 29) were: mitoxantrone, 12 mg/m2 every three weeks (total dose, 96 mg) and methothrexate, 35 mg/m2 every three weeks (total dose, 280 mg).
Contraindicatons Renal impairment (withdraw if renal impairment suspected; Appendix 7d); withdraw if tssue hypoxia likely (for example sepsis best 20mg sarafem women's health magazine weight loss tips, respiratory failure order 20 mg sarafem mastercard menstruation frequent urination, recent myocardial infarcton, hepatc impairment), use of iodine-containing X-ray contrast media (do not restart metormin untl renal functon returns to normal) and use of general anaesthesia (suspend metormin 2 days beforehand and restart when renal functon returns to normal); alcohol dependence; pregnancy (Appendix 7c); anaemia; ketosis. Precautons Measure serum creatnine before treatment and once or twice annually during treatment; substtute insulin during severe infecton; trauma, surgery (see notes above and contraindicatons); lactaton (Appendix 7b); interactons (Appendix 6a, 6b, 6c); hepatc or renal disease (Appendix 7a); heart disease. Adverse Efects Anorexia, nausea and vomitng, diarrhoea (usually transient), abdominal pain, metallic taste; lactc acidosis most likely in patents with renal impairment (discontnue); decreased vitamin B12 absorpton. Contraindicatons Hypersensitvity, type 1 diabetes, diabetc ketoacidosis, symptomatc or history of heart failure, children, lactaton. Precautons Oedema, congestve heart failure, hepatc dysfuncton, anaemia, concomitant oral contraceptves and hormone replacement therapy, pregnancy (Appendix 7c), interactons (Appendix 6c). Storage Store protected from heat, light and moisture at a temperature not exceeding 30⁰C. It induces gonadotrophin release by occupying estrogen receptors in the hypothalamus, thereby interfering with feedback mecha- nisms. Patents should be carefully counselled and should be fully aware of the potental adverse efects, including a risk of multple pregnancy (rarely, more than twins), of this treat- ment. Most patents who are going to respond will do so to the frst course; 3 courses should be adequate; long-term cyclical therapy (more than 6 cycles) is not recommended as it may increase risk of ovarian cancer. Dose Oral Adult- Anovulatory infertlity: 50 mg daily for 5 days, startng within 5 days of onset of menstruaton, preferably on the second day, or at any tme if cycles have ceased; a second course of 100 mg daily for 5 days may be given in the absence of ovulaton. Contraindicatons Hepatc impairment (Appendix 7a); ovarian cysts; hormone dependent tumours or uterine bleeding of undetermined cause; pregnancy (exclude before treatment, Appendix 7c); hyperprolactnaemia; depression. Precautons Visual disturbances (discontnue and initate eye examinaton) and ovarian hyperstmu- laton syndrome (discontnue treatment immediately); polycystc ovary syndrome (cysts may enlarge during treatment); uter- ine fbroids, ectopic pregnancy, incidence of multple births increased (consider ultra- sound monitoring); lactaton (Appendix 7b). Adverse Efects Visualdisturbances;ovarianhyperstmulaton; hot fushes; abdominal discomfort; occasional nausea and vomitng; depression; insomnia; breast tenderness; headache; intermenstrual spotng; menorrhagia; endometriosis; convulsions; weight gain; rashes; dizziness and hair loss. Proges- terone is relatvely inactve following oral administraton and produces local reactons at site of injecton. This has led to the development of synthetc progestogens including levonorg- estrel, norethisterone and medroxyprogesterone. Where endometriosis requires drug treatment, it may respond to synthetc progestogens on a contnuous basis. In post- menopausal women receiving long-term estrogen therapy for hormone replacement, a progestogen needs to be added for women with an intact uterus to prevent hyperplasia of the endometrium. Progestogens are also used in combined oral contraceptves and progestogen-only contraceptves. Dose Oral Adult- Endometriosis: 10 mg daily startng on ffh day of cycle (increased if spotng occurs to 20 to 25 mg daily, reduce once bleeding has stopped). Menorrhagia: 5 mg three tmes daily for 10 days to stop bleeding; to prevent bleeding 5 mg twice daily from day 19 to 26 of cycle. Contraindicatons Pregnancy (Appendix 7c); undiagnosed vaginal bleeding; hepatc impairment or actve liver disease (Appendix 7a); severe arterial disease; breast or genital tract cancer; porphyria; history in pregnancy of idiopathic jaundice, severe pruritus. Precautons Epilepsy; migraine; diabetes mellitus; hypertension; cardiac or renal disease and those susceptble to thromboembolism; depression; lactaton (Appendix 7b). These include oxytocic drugs used to stmulate uterine contractons both in inducton of labour and to control postpartum haem- orrhage and β2-adrenoceptor agonists used to relax the uterus and prevent premature labour. Postpartum Haemorrhage: Ergometrine and oxytocin difer in their actons on the uterus. In moderate doses oxytocin produces slow generalized contrac- tons with full relaxaton in between; ergometrine produces faster contractons superimposed on a tonic contracton. Oxytocin is now recommended for routne use in postpartum and post-aborton haemorrhage since it is more stable than ergometrine. However, ergometrine may be used if oxytocin is not available or in emergency situatons. Premature Labour: Salbutamol is a β2-adrenoceptor agonist which relaxes the uterus and can be used to prevent premature labour in uncomplicated cases between 24 and 33 weeks of gestaton. The greatest beneft is obtained by using this delay to administer cortcosteroid therapy or to implement other measures known to improve perinatal health.
|